Treatment for TTTS varies depending on the stage and severity of the disease. Options include:
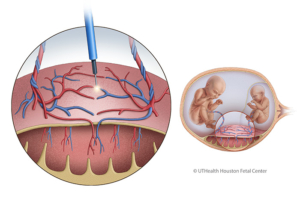
- Fetoscopic selective laser ablation
This minimally invasive procedure is the preferred treatment for moderate to severe TTTS. Using a fetoscope and laser, the shared blood vessels on the placenta are clotted to stop the abnormal blood exchange. This intervention improves survival rates, with at least one twin surviving in up to 90% of cases and both twins in 74%. Adverse neurological development occurs in around 14% of TTTS cases. - Selective cord occlusion
In severe cases where one twin is unlikely to survive, selective cord occlusion may be performed to protect the healthier twin. This procedure, though rarely used, prevents complications like neurological impairment in the surviving twin. - Expectant management
For mild cases (e.g., Stage 1), close monitoring with frequent ultrasounds is often sufficient to evaluate the progression of the disease. - Amnioreduction
Amnioreduction involves removing excess amniotic fluid from the recipient twin’s sac to reduce maternal discomfort and prolong the pregnancy. However, this is a temporary solution as fluid often reaccumulates, requiring repeated procedures.